Late last year I wrote a peace congratulating the Kenyan government and all those involved of having done a commendable job in reducing the HIV prevalence rate to 5.1%. But new figures out indicate that things are much worse than this. It turns out that the prevalence rate is 7.4% with about 1.4 million Kenyans between the ages of 15 and 64 infected.
Even more worrying is the fact that more than 83% of those infected do not know that they’ve been infected and less than half of them use condoms. The new figures also reported that 10% of married couples in Kenya are infected.
It goes without mention that this should sound an alarm among Kenyans. The truth needs to be put out there. It is true that Kenyan men, and to some extent women, are behaving badly. It is also true that they are not using condoms while at it.
What needs to be done is (I am no expert but this is sort of common sense):
1. The public should be educated bluntly about proper sexual behavior. There is no point in acting like people are not having indiscriminate sex while they are. Men especially should be constantly reminded that they should not be putting their families in danger by their bad habits.
2. Condoms. Condoms. Condoms. I don’t care what the church says. People are having sex. Abstinence is, I concede, the best prevention method. But what do you when people, in their fallibility cannot put down the natural urge to have sex? I say the government should avail condoms, not just to teenagers but to married men as well.
3. Empower women. Empower women. Empower women. Empowered women will be able to say no to unprotected sex. Empowered women will not be forced to have sex in exchange for food on the table for their children. Empowered women will raise well mannered, morally upright children who will not grow into deviants running around having indiscriminate sex.
EMPOWERED WOMEN WILL PROVIDE A SOUND FOUNDATION TO SOCIETY.
These are just three things that the government can do to prevent the figures rising further than 7.4%. They may seem sort of naive, but the truth is they are achievable. They are achievable if the folks in Nairobi behaved like the leaders they ought to be and strove at changing society – for this is part of leadership. Kenya and indeed African leaders can change the course of this terrible disease if they want to.
Some of them like our dear president have more than one wife (or some other hazy definition – partner, wife, concubine etc). What message are we sending to the young. When leaders are allowed to run around having illegitimate children we set a bad example. It should start with leaders having responsible sexual relations and then preaching to the masses to have responsible sexual relations.
Otherwise millions more will die. Millions more will be orphaned. And millions that could have been spent building roads and schools will instead be spent on funerals and health costs.




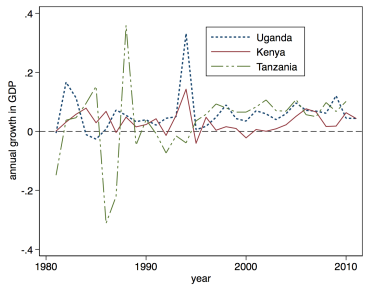 Uganda’s post civil war economic recovery may have been impressive (see graph), but it should no longer be something for Museveni to hang his hat on. It is clear that the longer Museveni stays in office, the more he is going to undo his very own achievements in the earlier years of his three-decade rule.
Uganda’s post civil war economic recovery may have been impressive (see graph), but it should no longer be something for Museveni to hang his hat on. It is clear that the longer Museveni stays in office, the more he is going to undo his very own achievements in the earlier years of his three-decade rule.