It is quite a shame that the church is somewhat contributing to the spread of the HIV virus on the continent of Africa. Church leaders, especially of the Catholic variety, have always maintained that the use of contraceptives – including condoms – is against the will of God. Given Africans’ religiosity and respect for these men of God, many of them have ended up not using any form of protection or contraceptives while having sex. The result has been the very high fertility and HIV infection rates on the continent.
African governments have been fighting the AIDS scourge with very costly campaigns while turning a deaf year to the churches.Because in most cases the churches are the ones that provide much needed public goods and social services, they’ve come to have a stronger grip on the people’s minds and hearts than the government. It is therefore a no brainer that even on the life and death issue of condom use they tend to listen more to the men of God than to Caesar.
This should not be the case. To echo Wole Soyinka, “Even in a purely theocratic state, there comes a point – surely – at which the state must restrict clerical interference in clearly scientific matters, most especially where human well being and survival are at issue.” Although the percentage of those infected because of their religious persuasions may be small, the fact is that their infection is preventable. It is because of this that governments should step in and rid pulpits of this madness. Church leaders should stop deluding themselves that their call for abstinence is in God’s people’s interest.The truth is that God’s people will always have sex and therefore need ways to control their fertility and protect themselves against terrible sexually transmitted diseases.
This does not mean that the churches should stop preaching about chastity and sexual purity. On the contrary, I say they should redouble their effort. But they should also be flexible on contraceptives, including condoms, for the safety of the many of their flock who fall to the temptations of the flesh.
The continent’s men of God should take time off next time they are in Rome, London or Texas – from where they get their cue – to inquire about the rates of condom use and fertility of their fellow believers in these places.




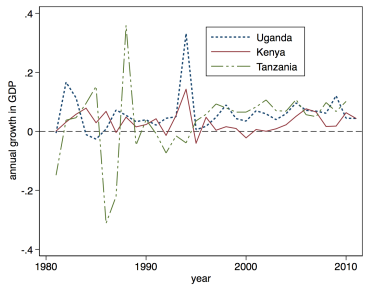 Uganda’s post civil war economic recovery may have been impressive (see graph), but it should no longer be something for Museveni to hang his hat on. It is clear that the longer Museveni stays in office, the more he is going to undo his very own achievements in the earlier years of his three-decade rule.
Uganda’s post civil war economic recovery may have been impressive (see graph), but it should no longer be something for Museveni to hang his hat on. It is clear that the longer Museveni stays in office, the more he is going to undo his very own achievements in the earlier years of his three-decade rule.